
HIP DISLOCATION
Children with hip dislocations are either congenital or traumatic. Congenital hip dislocation (CHD) is a condition in which a child is born with an unsteady hip. Traumatic injury is the result of an accident or a large force that causes a hip to dislocate.
At the Medical City Children’s Orthopedics and Spine Specialists medical practice, our expert Hip Dislocation Doctors and surgeons are dedicated to diagnosing and treating children with all types of medical conditions to ensure comprehensive care is tailored to each patient’s needs. We only specialize in children’s health, and we have undergone advanced training to do so. We treat minor and very major medical conditions with a compassionate approach, and our team cares for patients suffering from Hip Dislocation.
If your child needs surgery or casting, our Fracture Care Clinic opens every day and you do not need an appointment. Surgery rooms get scheduled every morning, so your child receives the care and attention they need right away.
Hip Dislocation
 Hip dislocations found in children are either congenital or traumatic. Congenital dislocation of the hip is the result of dysplasia of the femoral head or acetabulum. Congenital hip dislocation (CHD) is a condition in which a child is born with an unstable hip. It’s the result of abnormal formation of the hip joint that happens during the early stages of fetal development. This condition is also known as “developmental dysplasia of the hip” (DDG). And as your child grows, this instability worsens.
Hip dislocations found in children are either congenital or traumatic. Congenital dislocation of the hip is the result of dysplasia of the femoral head or acetabulum. Congenital hip dislocation (CHD) is a condition in which a child is born with an unstable hip. It’s the result of abnormal formation of the hip joint that happens during the early stages of fetal development. This condition is also known as “developmental dysplasia of the hip” (DDG). And as your child grows, this instability worsens.
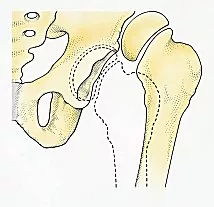
In the child’s hip, the ball-and-socket joint may sometimes dislocate. Clearly, this means that with movement, the ball will slip out of the socket. Sometimes, the joint may even dislocate completely.
On the other hand, Traumatic hip dislocation is an orthopedic emergency. Certainly, large forces are necessary to cause a hip dislocation like this. As a result, other injuries may have occurred, including severe injuries and fractures. Even though Hip Dislocation is painful, proper and fast diagnosis and the right medical management can reduce suffering.
The doctors at Medical City Children’s Orthopedics and Spine Specialists are highly skilled and experts at diagnosing and treating hip disorders.
CHD Cause
In many cases, the cause of CHD is unknown. The contributing factors are low levels of amniotic fluid in the womb and breech presentation, in which your baby is born hips first. While there might be a family history of the condition, confinement in the uterus may cause CHD. That is why a baby is more likely to have this condition if a woman is pregnant for the first time. It is because here the uterus hasn’t been stretched previously.
Even though any infant can have the condition, CHD is more common in girls than in boys. A doctor routinely checks your newborn for any signs of hip dislocation. During their first year of life, experts also keep examining your child’s hips.
Traumatic Hip Dislocation
The most common cause of this type of hip dislocation is direct trauma, especially road traffic accidents and falls.
- Children may sustain hip dislocation even from minor trauma.
- Traumatic hip dislocations are often the result of motor vehicle accidents or significant falls from height.
- People often easily overlook hip dislocations if there is a related femur fracture.
- Experts need to manage and reduce hip dislocations in children gently to avoid injury to the femoral epiphysis.
- Traumatic dislocations may be of three types: posterior, anterior, or central.
Posterior Dislocation of The Hip
This occurs because of a major force on a flexed knee and hip. This can also cause other serious injuries, such as fractures of the posterior acetabulum or femur. Doctors usually make the diagnosis with an AP X-ray.
Posterior hip dislocation is a common form of hip injury, typically resulting from high-impact trauma, such as car accidents or falls. The force applied to the knee when the hip is flexed is the primary mechanism leading to dislocation.
QUESTIONS AND ANSWERS
What causes hip dislocation in children?
Hip dislocation in children can occur due to various causes, including:
- Congenital Hip Dysplasia: This refers to a common cause, where the hip joint doesn’t develop properly, making it prone to dislocation.
- Trauma: A direct blow or forceful impact to the hip region, such as in a car accident or a fall, can dislocate the hip.
- Developmental Issues: Conditions like cerebral palsy or muscular dystrophy can lead to muscle imbalances that may contribute to hip dislocation.
- Genetic Factors: Some children may have a genetic predisposition to hip instability or dislocation.
How do doctors diagnose and treat hip dislocation in children?
Diagnosis and treatment of hip dislocation in children involve the following steps:
- Clinical Examination: A healthcare provider will perform a physical examination, looking for signs of hip instability, asymmetry, and limited range of motion.
- Imaging: X-rays are typically used to confirm the diagnosis and assess the severity of the dislocation. Ultrasound may be used in infants to evaluate hip dysplasia.
- Treatment: The treatment approach depends on the cause and severity of the dislocation:
- Non-Surgical Methods: In some cases, especially with congenital hip dysplasia, non-surgical methods like the use of a Pavlik harness or a spica cast may be effective in repositioning the hip joint.
- Closed Reduction: If the hip becomes dislocated, but the bones are still aligned, a closed reduction procedure may be performed to manipulate the joint back into its proper position under anesthesia.
- Surgery: Doctors recommend surgical intervention for severe hip dislocations or when conservative methods fail. Surgical procedures may involve open reduction, osteotomies, or other techniques to stabilize the hip joint.
- Rehabilitation: After treatment, rehabilitation and physical therapy are essential to help the child regain hip joint function and prevent recurrence.
In addition to pediatric cases, hip dislocation management in clinical practice also encompasses a wide array of considerations for different populations:
- Traumatic Hip Dislocation: Often seen in adults and athletes, this condition requires immediate attention. Clinical guidelines recommend early intervention to minimize complications. Closed reduction is commonly used, followed by imaging to confirm alignment.
- Developmental Dislocation (Dysplasia) of the Hip (DDH): This condition is particularly prevalent in infants and young children. It may necessitate early screening and intervention to prevent long-term joint issues.
- Advanced Imaging Techniques: While X-rays are standard, MRI and CT scans may be employed in complex cases to assess soft tissue damage or in post-operative evaluations.
- Outcome Measures: Various scoring systems, such as the Harris Hip Score, are utilized to evaluate hip function and track recovery progress.
- Research Insights: Studies highlight the importance of timely diagnosis and personalized treatment plans to ensure optimal recovery and reduce the risk of recurrence or joint degeneration over time.
By integrating these comprehensive strategies, healthcare providers can effectively manage hip dislocation across all age groups, ensuring tailored care that aligns with the latest clinical research and guidelines.
What are the potential complications and long-term effects of hip dislocation in children?
Hip dislocation can lead to various complications and long-term effects, including:
- Chronic Pain: Untreated or improperly managed hip dislocations can result in chronic pain and discomfort.
- Gait Abnormalities: Hip instability and dislocation can affect a child’s walking pattern and may lead to long-term gait abnormalities.
- Early-Onset Arthritis: Hip dislocation can increase the risk of developing early-onset hip arthritis in adulthood.
- Functional Limitations: Depending on the severity and treatment success, some children may experience long-term functional limitations or mobility challenges.
- Hip Dysplasia: Hip dysplasia may persist or develop as a consequence of hip dislocation, requiring ongoing monitoring and treatment.
Early diagnosis and appropriate treatment are crucial to minimize complications and optimize outcomes for children with hip dislocation. Timely intervention can help ensure the best possible hip joint function and quality of life.
Common Causes
- Motor Vehicle Accidents: The most frequent cause is when the knee hits the dashboard, driving the femur backward.
- Falls: High-impact falls, particularly in older adults, can result in this type of dislocation.
- Sports Injuries: Contact sports can also lead to such injuries due to sudden, forceful impacts.
Diagnosis and Treatment
- X-ray Imaging: An AP X-ray is crucial for confirming the dislocation and assessing any accompanying fractures.
- Closed Reduction: Typically, the first line of treatment, where the dislocated hip is manually repositioned by a healthcare professional.
- Surgical Intervention: Required if there are associated fractures or if closed reduction is unsuccessful.
- Rehabilitation: Involves physiotherapy to restore mobility and strengthen the hip joint post-treatment.
Long-term Management
- Monitoring for Complications: Such as avascular necrosis or osteoarthritis, which may develop if the blood supply to the femoral head is compromised.
- Regular Follow-ups: Essential to ensure proper healing and prevent future dislocations.
This comprehensive approach to understanding posterior hip dislocation helps in both preventing future injuries and managing existing conditions effectively.
Anterior Dislocation of the Hip
This injury is less common. It causes pain in the hip and causes an inability to walk or move the leg. The leg rotates externally, abducts, and extends at the hip. The initial treatment is to provide analgesia, the reduction under general anesthesia, etc.
Considerations for Traumatic Hip Dislocation in Athletes
When dealing with traumatic hip dislocations in athletes, there are several critical considerations to ensure effective treatment and successful recovery:
- Immediate Medical Attention
- Prompt Reduction: It’s essential to reduce the dislocated hip as quickly as possible to minimize potential complications, such as avascular necrosis.
- Stabilization: Ensuring the joint is stabilized post-reduction is crucial to prevent further injury.
- Comprehensive Assessment
- Imaging: Use X-rays or MRI scans to evaluate the extent of the injury, checking for associated fractures or soft tissue damage.
- Range of Motion and Strength Testing: Assess the athlete’s range of motion and strength before devising a rehabilitation plan.
- Individualized Rehabilitation Program
- Gradual Return to Activity: An incremental approach is recommended, progressively increasing load and complexity of activities.
- Physical Therapy: Tailored exercises that restore flexibility, strength, and stability in the hip region to ensure full recovery.
- Prevention of Future Injuries
- Technique Adjustments: Coaching on proper techniques and movements can reduce the risk of recurrence.
- Protective Gear and Equipment: Evaluate the use of protective gear and adapt equipment as necessary to enhance safety.
- Psychological Support
- Mental Readiness: Address any psychological barriers the athlete may face when returning to their sport.
- Support Systems: Leverage sports psychologists or support groups to aid in the athlete’s mental recovery.
Thompson-Epstein Classification System
These considerations are key to dealing with the immediate effects of a traumatic hip dislocation and ensuring long-term health and performance sustainability for athletes.
The Thompson-Epstein classification system is a key method used to categorize posterior traumatic hip dislocations, specifically focusing on the types and severity of associated fractures. Here’s a breakdown of the system:
I: Simple Dislocation
- Involves a basic dislocation that may or may not include a minor fragment from the posterior wall. The fragment, if present, is typically insignificant and does not complicate the injury further.
II: Large Posterior Wall Fragment
- Characterized by a dislocation that includes a substantial fragment from the posterior wall. This fragment is significant enough to impact the stability and treatment approach.
III: Comminuted Posterior Wall Fragment
- This type involves a dislocation where the posterior wall fragment is highly fragmented or broken into several pieces, presenting a more complex scenario for treatment and recovery.
IV: Acetabular Floor Fracture
- In this category, the dislocation is accompanied by a fracture of the acetabular floor, which is the socket portion of the hip joint. This adds another dimension of complexity for orthopedic intervention.
V: Femoral Head Fracture
- The most intricate type, as it includes a dislocation along with a fracture of the femoral head itself, necessitates a nuanced and often more invasive approach to treatment.
Each type signifies an increasing level of complexity and injury severity, guiding medical professionals in diagnosing and deciding on appropriate treatment plans.
Central Dislocation of the Hip
This condition happens when a fall or force is put along the length of the femur, and the head of the femur drives through the fractured acetabular floor. The level of leg deformity depends on the extent and nature of penetration into the pelvis. The leg shortens, abducts, or adducts, and rotates internally or externally. For diagnosis, our doctors usually use an AP pelvic X-ray.
CHD Symptoms
CHD may have no symptoms. That is why specialists will routinely test your child for the condition. If your child has this condition, the common symptoms are:
- Legs that turn outward or seem different in length
- Restricted motion
- Folds on the legs and buttocks that appear uneven when the legs extend
- Delayed development of gross motor skills, which impacts the way your child sits, crawls, and walks
Hip Dislocation Diagnosis
Screening for CHD generally happens at birth and also occurs throughout the first year of your child’s life. Furthermore, a physical exam is the most common screening method. Hence, the doctor will gently move and check your child’s hip and legs to look for any clicking or clunking sounds. Such a sound may indicate a dislocation. This exam comprises two tests:
- Ortolani test – During this test, your child’s orthopedic doctor will apply upward force to move your child’s hip away from the body. The movement away from the body is abduction.
- Barlow test – In this test, your child’s doctor will apply a downward force to move your child’s hip across the body. Applying force toward the body is adduction.
These tests are only appropriate before your child is 3 months old. In older babies and children, findings that help indicate CHD are limited abduction, limping, and different leg lengths if a single hip is affected.
Imaging tests can help confirm a CHD diagnosis. Doctors use ultrasounds for babies who are younger than 6 months old. They utilize X-rays for examining older babies and children.
The Importance of Timely Hip Dislocation Relocation
When dealing with a traumatic hip dislocation, speed is crucial. Prompt relocation is not merely a suggestion; it’s a significant factor in minimizing potential complications. Acting swiftly within a certain time frame, typically within six hours, is essential to prevent serious issues.
Why Timing Matters:
- Preventing Nerve Damage: Delayed relocation can increase the risk of nerve injuries, particularly to the sciatic nerve. Early intervention helps safeguard against this.
- Reducing the Risk of Avascular Necrosis: The hip joint relies heavily on its blood supply. Prolonged dislocation can impair circulation, leading to avascular necrosis, where bone tissue dies due to a lack of blood flow.
- Minimizing Joint Damage: Immediate relocation can decrease the likelihood of permanent joint damage and the need for more invasive procedures later.
- Facilitating Faster Recovery: Quick action enhances recovery prospects, allowing for better rehabilitation outcomes and a swifter return to normal activities.
- Limiting Soft Tissue Injury: The longer a dislocation remains untreated, the greater the potential damage to surrounding muscles and ligaments.
The takeaway? Swift relocation is not merely beneficial; it’s a critical step in ensuring the best possible recovery from a traumatic hip dislocation. This strategy ensures that patients not only reduce the risk of complications but also improve their long-term mobility and quality of life.
Treatment of Hip Dislocation
If your baby, younger than 6 months of age, has CHD, it is quite likely that the child will be fit for a Pavlik harness. This harness helps press the hip joints into the sockets. The harness plays a crucial role in abducting the hip by securing the legs in a frog-like posture. Depending on the age of the child and the severity of the condition, your baby may have to wear this harness for 6 to 12 weeks full-time or part-time.
If the treatment with a Pavlik harness appears unsuccessful, or your baby is too big to fit in the harness, your doctor may recommend surgery. Subsequently, surgeons perform the procedure under general anesthesia. Sometimes, this may involve simply maneuvering their hip into the socket. This procedure is called a closed reduction.
Also, the surgeon may surgically lengthen the tendons of your baby and eliminate other obstacles before repositioning the hip. This procedure is called an open reduction. After repositioning your baby’s hip, their hips and legs will stay in casts for at least 3 months. However, if your child hasn’t responded well to treatment or is 18 months or older, he may need femoral or pelvic osteotomies to reposition the hip. In this method, a surgeon will reshape or divide the acetabulum of the pelvis (the hip socket) or the head of the femur (the ball of the hip joint).
Physiotherapy for Hip Dislocation
When managing physiotherapy for patients with hip dislocation, several key components are fundamental to effective recovery:
Initial Assessment and Planning
- Assessment of Injury: Understanding the extent of soft tissue and bone involvement is crucial. This often requires close collaboration with an orthopedic surgeon to determine any weight-bearing restrictions.
- Personalized Plan Development: Create a rehabilitation program tailored to the individual’s specific needs, considering both soft tissue and bone healing timelines.
Impact of Traumatic Hip Dislocations on Long-Term Quality of Life and Functionality
Traumatic hip dislocations can have a profound impact on an individual’s long-term quality of life and overall functionality. Here’s how:
Long-Term Quality of Life
- Chronic Pain: Persistent discomfort can plague those who have experienced a hip dislocation. This ongoing pain often affects daily activities, making even simple tasks challenging.
- Reduced Mobility: The ability to move freely can be significantly impaired. This restriction may lead to a reliance on mobility aids or modifications in one’s environment to accommodate decreased movement capabilities.
- Psychological Effects: The limitations imposed by hip dislocations can lead to feelings of frustration, depression, or anxiety. The ongoing struggle to adapt to new physical limitations can affect mental health, contributing to an overall diminished sense of well-being.
Functionality and Physical Capabilities
- Limited Range of Motion: Dislocations can result in a decreased range of motion in the hip joint, impacting one’s ability to perform actions such as bending, walking, or climbing stairs.
- Muscle Weakness: Post-injury, muscle strength around the hip may deteriorate, reducing the ability to perform weight-bearing activities effectively.
- Increased Risk of Osteoarthritis: The trauma from a hip dislocation can accelerate the development of osteoarthritis, further impacting joint functionality and leading to additional health concerns as the individual ages.
- Need for Rehabilitative Measures: Many individuals require ongoing physical therapy to regain strength and improve flexibility.
Evaluating Outcomes
Clinical evaluations use several metrics to assess the impact on functionality:
- Harris Hip Score (HHS): This is a well-established method to evaluate hip function, focusing on pain levels, mobility, and need for pain medication.
- Hip Disability and Osteoarthritis Outcome Score (HOOS): This score assesses symptoms and function related to hip osteoarthritis, providing insights into the daily life impact.
- Oxford Hip Score (OHS): A patient-reported score that highlights perceived pain and movement issues related to hip function post-injury.
- Lequesne Index of Severity for Osteoarthritis of the Hip (LISOH): Evaluates pain, maximum walking distance, and activities of daily living to determine severity.
- AAOS Hip and Knee Questionnaire: Offers a comprehensive picture of joint function, capturing details beyond the hip to offer a broader assessment of overall quality of life and physical capabilities.
Overall, traumatic hip dislocations have a substantial effect on life quality. Their impact on both physical function and mental health requires a multidisciplinary approach to management and rehabilitation to help individuals regain as much functionality and comfort as possible.
Core Rehabilitation Elements
- Gait Re-education:
- Begin with assistive devices like crutches or a walker to limit weight-bearing. Gradually reduce dependence on these aids as the patient’s strength and stability improve.
- Range of Motion Enhancement:
- Incorporate hip mobilization exercises to safely increase the flexibility and range of motion of the joint.
- Muscle Strengthening:
- Focus on strengthening exercises for the surrounding muscles, particularly the hip stabilizers such as abductors, adductors, extensors, and flexors.
- Stretching:
- Implement daily stretching routines to maintain muscle elasticity and prevent stiffness.
- Controlled Activity Resumption:
- Introduce a graded approach to returning to everyday activities or sports, ensuring that increases in activity levels are cautious and guided.
Progress Monitoring
- Regularly evaluate the patient’s progress and adjust the therapy plan as needed. Continuous monitoring ensures that rehabilitation aligns with the patient’s healing process and any evolving medical guidance.
By adhering to these components, patients are better positioned to achieve complete recovery in a timeframe typically spanning 3 to 6 months.
The Crucial Role of Physiotherapy in Hip Dislocation Rehabilitation
Physiotherapy is essential for recovery after a hip dislocation. When a hip is dislocated, it’s not just about putting it back into place; it’s about ensuring a complete return to daily activities and preventing future issues. Here’s how physiotherapy contributes to this process:
- Restoring Mobility: One of the primary goals of physiotherapy is to regain the normal range of motion in the hip joint. Through carefully designed exercises, a physiotherapist helps improve flexibility and reduce stiffness.
- Strength Building: Strengthening the muscles around the hip joint is vital. Physiotherapy involves exercises that target these areas, helping to stabilize the joint and reduce the risk of further injury.
- Pain Management: Therapeutic techniques, including manual therapy and modalities like heat or cold therapy, can help manage pain and swelling, making the rehabilitation process more comfortable.
- Functional Training: Beyond basic movement, physiotherapy includes training on specific tasks and activities. This ensures that patients can confidently return to their normal routines and favorite activities.
- Preventative Strategies: Physiotherapists offer guidance on posture, balance, and movement techniques to minimize the chances of recurring dislocations.
Overall, physiotherapy is not just about healing the hip, but empowering individuals to regain their independence and achieve a better quality of life post-injury.
Prevention
Unfortunately, parents cannot prevent CHD. It’s crucial to take your child with this condition to regular checkups. This is how the doctors can identify and treat the condition ASAP.
The long-term outlook
When the doctor identifies CHD earlier, and your baby gets treatment with a Pavlik harness at the right time, complicated invasive treatment is not likely to be necessary. According to the experts, around 80 to 95 percent of cases that are identified early get successful treatment. And the treatment is determined by the seriousness of the condition.
The success rate might vary from one surgical treatment to another. While some treatments only require one procedure, others may need multiple surgeries and years of proper monitoring. If your child’s CHD does not get proper treatment in early childhood, it can lead to early arthritis and severe pain in the future. And in serious cases, even total hip replacement surgery might be necessary. Even if your child’s CHD treatment is successful, they must keep visiting an orthopedic specialist regularly to ensure the problem doesn’t come back and that their hip continues to grow properly.
Conclusion
When it comes to treating congenital and traumatic hip dislocations, the sooner the diagnosis, the better. Consulting trusted orthopedic doctors like those at the Medical City Children’s Orthopedics and Spine Specialists will help you properly diagnose the condition and get the best treatment accordingly. To make it convenient for our patients, we have offices in Arlington, Dallas, Flower Mound, Frisco, and McKinney, TX. Finally, we are accepting new patients and invite parents to give us a call and make an appointment.
___________________
Citation: The Royal Children’s Hospital: Hip Dislocation
The medical content on this page has been carefully reviewed. It was approved for accuracy by the Medical City Children’s Orthopedics and Spine Specialists’ qualified healthcare professionals. This includes our board-certified physicians and Physician Assistants. Our team ensures that all information reflects the latest evidence-based practices and meets rigorous standards of medical accuracy, with oversight from our expert spine doctors to guarantee the reliability of our information for our patients.
Call 214-556-0590 to make an appointment.
Comprehensive services for children from birth through adolescence at five convenient locations: Arlington, Dallas, Flower Mound, Frisco and McKinney.